A patient guide to physiotherapy for total hip replacement (hip arthroplasty) surgery

Mr Sanjeev Patil- Orthopaedic Hip Specialist
Frank Gilroy- Senior Physiotherapist
Megan Thea Ross Browne- Student Physiotherapist
Contents
- Hip anatomy
- Movements of the hip
- Why you may require a hip replacement
- About the procedure
- Surgical techniques
- What to expect following surgery
- Rehabilitation
- Pre-operative rehabilitation
- Post-operative rehabilitation:
- Immediate post-operation: day 0-2
- Phase 1: weeks 1-2
- Phase 2: weeks 3-6
- Phase 3: weeks 7-12
- Phase 4: week 12 onwards
- Frequently asked questions:
- Return to activity
- Return to work
- References
Remember this programme is only a guideline. You may progress more rapidly or slowly through the programme as guided by your Surgeon and Physiotherapist. You should always check with them before progressing onto the next rehabilitation stage.
Anatomy of the Hip
The hip is a synovial ball-and-socket joint formed between the acetabulum of the pelvis and the head of the femur (thigh bone). Functionally, the hips are the main joints that connect the trunk to the lower limbs and therefore need to have enough stability to withstand body weight in a variety of positions.
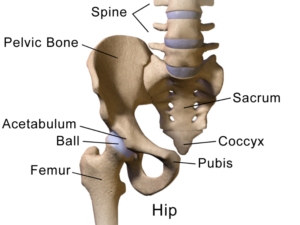 Bones of the hip and pelvis
Bones of the hip and pelvis
The hip achieves its stability through the anatomical structures that surround it and through the design of the joint itself.
Anatomical features contributing to the stability of the hip include:
- The shape of the acetabulum- creates a deep socket which encloses the majority of the femoral head
- Acetabular labrum– a ring of fibrous cartilage that attaches around the outside of the acetabulum, increasing the depth of the socket
- Strong surrounding ligaments– attach bone to bone and limit excessive movement at the hip
- Synovial membrane– lines and covers all non-articular surfaces, producing synovial fluid to lubricate and reduce friction within the joint
- Surrounding muscles– (glutes, iliopsoas, hamstrings, quadriceps, short lateral rotators, abductors and adductors) work in coordination to stabilise the joint
 Anatomical features of the hip joint
Anatomical features of the hip joint
Movements of the hip
The structure of the hip and the muscles surrounding it enable the joint to be capable of moving in 6 different motions. All of these movements are essential for daily activities such as walking, sitting or playing sports.
The 6 possible movements of the hip are:
- Flexion and extension
- Abduction and adduction
- External and internal rotation

Why you may require a hip replacement
A total hip replacement (also known as a total hip arthroplasty) may be required for a number of different reasons or conditions including:
- advanced arthritis
- developmental hip dysplasia
- hip fractures or joint damage caused by trauma
The most common condition that leads to someone requiring surgery is advanced osteoarthritis (OA).
OA of the hip is a condition where the articular cartilage that covers and protects the bony surfaces of the hip joint- allowing them to glide smoothly against one another- becomes thinner and damaged. This can cause the bone ends underneath to become exposed, rough and misshapen and lead to pain, stiffness and reduced movement within the joint.
Individuals with OA may notice stiffness and a reduction in range and ease of movement, reduced hip/leg strength and changes to their walking pattern (often developing a limp to try and offload the painful joint).
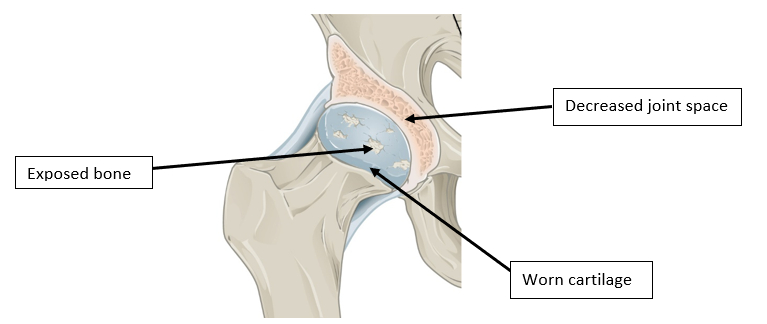 Osteoarthritis of the hip
Osteoarthritis of the hip
Non-operative (conservative) treatments such as physiotherapy, weight loss, walking aids and steroid injections will be recommended and used before surgical intervention. Your specialist may perform an x-ray and/or MRI/CT scan to guide treatment and detect changes within the hip joint. Surgery could be recommended when conservative treatments no longer relieve your pain. The decision to have a total hip replacement will be a joint discussion and decision between yourself and your specialist.
The aim of the procedure is to reduce pain and increase mobility, with the goal of improving your functional abilities and quality of life.
About the procedure
A total hip replacement is a common surgical procedure during which the damaged hip joint socket and head of femur are removed and replaced with artificial components.
Different types of joint replacement can be used for the procedure and your specialist can discuss these with you further. The decision on what type you receive will depend on the degree of damage to your joint surfaces, your suitability for a particular type and your specialists’ preference.
The two sides of the replacement which move together-referred to as the bearing surface- can either be metal-metal, metal-plastic (polyethene) or ceramic-ceramic. The Surgeon will then use either a cemented or uncemented fixation to secure the components in place.
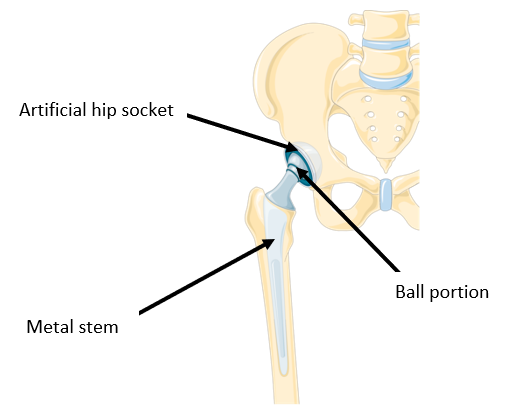
Total hip replacement components
Surgical techniques
The operation can be done under a general anaesthetic (putting you to sleep), or under a spinal anaesthetic (where you remain awake but will have no feeling below the waist). This decision will be made by your specialist and discussed with you beforehand. An epidural which is similar to a spinal anaesthetic can also be used.
The surgery involves an incision (cut) being made over the side of your hip of up to 30cm to allow the Surgeon to remove the damaged femoral head and hollow out the natural hip socket. A short, metal shaft with a smooth ball located on its upper end is placed into the hollow of your femur (thigh bone) and secured in place. An artificial socket will be fitted and secured into the space in your pelvis to form the hip socket. The operation can be done using different surgical techniques, including minimally invasive surgery. The type of surgery you receive will depend on your Surgeon and your suitability for a particular procedure.
What to expect following surgery
The aim of a total hip replacement is for you to regain increased function in your hip, which will hopefully enable you to return to normal daily activities with an improved range of movement and reduced pain. Completing your post-operative rehabilitation and participating in regular exercise will help you to gradually regain strength, movement and function in your hip. However, it is important you receive advice from your Surgeon and Physiotherapist on what they feel is achievable for your rehabilitation goals.

Modern artificial hip replacements are expected to last for at least 15 years however, this can vary between individuals and different types of replacements. The longevity of a hip replacement can be decreased if excessive stress is placed through the components for example, from manual work, running and high impact sports.
For a number of different reasons, after having a hip replacement your operative leg may appear longer or shorter than your other leg. Most patients adjust to this over time but a shoe raise can sometimes be required.
Rehabilitation
In general, after having a hip replacement healing takes around 3 months and full recovery about 18-24 months, however this can vary between individuals and different types of surgery. Factors that can affect how quickly you recover include your age, general fitness levels and the condition of your joints and muscles.
Physiotherapy before (pre-operative) and after (post-operative) joint replacement surgery is recommended by the National Institute for Health and Care Excellence (NICE) 2020 clinical guidelines.
The recovery process can be broken down into 4 phases:

IMPORTANT: before starting this programme, please note that:
- Progressions throughout the programme, between and within phases, should be made only when advised by your Physiotherapist
- If at any point during your programme you begin to experience pain, stop the exercise and consult your Physiotherapist
Pre-operative rehabilitation
Aim: to improve post-surgical outcomes by establishing a routine of regularly doing your physiotherapy exercises.
These exercises should be self-monitored and modified as appropriate because you want to be working at an intensity and for as long as you feel comfortable without aggravating your pain.
Aim to do these exercises 5 times per week, ideally starting 4-6 weeks before the surgery.
- Cardiovascular exercise
Complete 20-30 minutes (depending on your fitness) of either cycling, swimming or cross trainer before your exercises.
- For more athletic individuals this can be increased to 30-60 minutes
2. Hydrotherapy/pool work– the buoyancy of the water enables you to exercise without stress being applied to your joints. Ensure your Physiotherapist supervises you during the first session and that an aqua belt is worn to support you in the water.
Aim to complete a 20-30-minute pool session (depending on your fitness), 3-4 times per week:
- Aqua walking/jogging: use your arms and legs in the same motion as you would do on land.
- Mobility: complete 3 sets of 10 repetitions of the following exercises at the side of the pool (remaining in the water) whilst taking a rest in between sets of aqua walking/jogging.
- Hip flexion– bring your knee up towards your chest
- Hip extension– take your leg out behind you, keeping the knee straight
- Hip abduction– take your leg out to the side, keeping the knee straight
3. Mobility: aim to do 2-3 times per day
- Hip flexion in standing
- Stand upright with support
- Lift your knee up towards your chest
- Hold for up to 5 seconds, then relax
- Aim for 10-15 repetitions

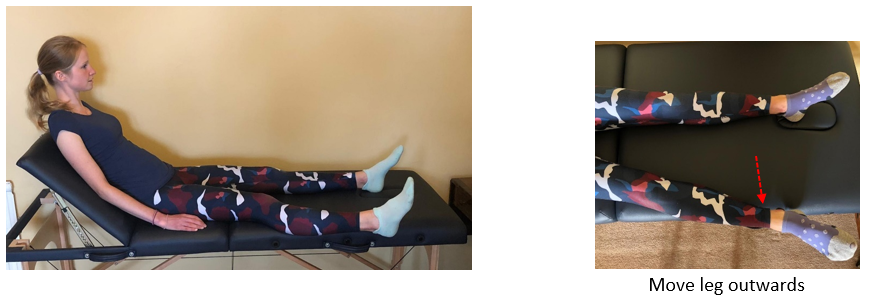
- Hip abduction in standing
- Stand upright with support
- Keeping your leg straight and toes pointing forwards, lift your leg out to the side as far as comfortable
- Hold for up to 5 seconds, then relax
- Aim for 10-15 repetitions

4. Strength: aim to do 2-3 times per day. These exercises should be done in long sitting with your back supported
- Static glutes
- Tense/squeeze your buttock muscles together
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Static quads
- Place a pillow or folded towel underneath your knee
- Gently press the knee in towards the bed by tensing your thigh muscles and bringing your toes back towards you
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Straight leg raise
- Keeping your toes pointing upwards, lift your leg straight up off the bed
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Inner range quads
- Place a rolled-up towel underneath your knee so the leg is slightly bent
- Keeping your toes pointing towards the ceiling, tense your thigh muscles to straighten your knee
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

5. Core exercises: aim to complete 2 times per day. Work towards being able to hold each exercise comfortably for more than 1 minute.
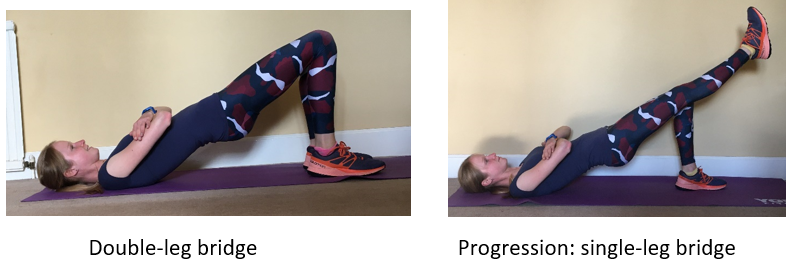
- Double-leg bridge
- Lie on your back with your knees bent
- Flatten the small of your back into the floor and lift your hips up by pushing through your heels
- Concentrate on keeping your hips level and body in a straight alignment

- Plank
- Starting on your forearms and knees
- Straighten out your legs to transfer the weight through your forearms and feet
- Concentrate on keeping your back straight by tightening your core muscles

Once you can comfortably hold the above core exercises for more than 1 minute, progressions can be found in Frank Gilroy’s Core strengthening programme by clicking here
Post-operative rehabilitation
The goals of post-operative rehabilitation are to restore your physical function and independence with activities of daily living.
After your operation, the muscles and tissues surrounding your hip replacement will take time to heal. It is therefore important that you follow certain precautions to avoid putting your hip into a position that could risk dislocation. Your Surgeon or Physiotherapist will advise you on these precautions and the length of time they must be followed for.
Precautions can include:
- Avoid bending your operative hip beyond 90 degrees (right angles)– for example, do not bend forward or down when sitting, avoid low chairs and don’t allow your knee to be in a position that is higher than your hip
- Avoid bringing your operative leg across the midline of your body– for example, don’t cross your legs when standing, sitting or lying
- Avoid turning or twisting your operative leg in towards your midline
- No running or jumping
- It can be advised that you continue to sleep on your back for the first 6 weeks after surgery
Immediately post-operation: Day 0-2
Aim: to be able to mobilise with assistance/crutches and gradually begin to work on range of movement.
- It is normal to experience some discomfort and fatigue when walking and doing your exercises initially and your ankles and feet may be swollen after the procedure.
Using your crutches: crutch use and the amount of weight you are allowed to place through your new hip is dependent upon your Surgeon’s opinion. Due to variations between individuals and types of surgery the duration of your crutch use is indeterminable.
- Your Physiotherapist will teach you the correct technique for using your crutches/walking aid.
- Circulation
- Ankle pumps and circles- increases the circulation in your legs to reduce the risk of a blood clot (DVT) in the blood vessels of the calf
- Long sit with your back supported and legs out straight
- Move your ankles backwards, forwards and in circular motions
- Aim to repeat 10-20 times, every 2 waking hours

2. Mobility
- Hip flexion- heel slides
- Long sit with your back supported and legs out straight
- Slide the foot of your operative leg up towards your bottom, allowing your knee and hip to bend- only go as far as comfortable. Do not bend your operative hip more than 90 degrees/ right angles
- Relax your foot back down to the starting position
- Repeat 15 times (or as pain allows) every 2 waking hours

- Hip Abduction
- Long sit with your back supported and legs out straight, keeping your toes pointing towards the ceiling
- Take your operative leg out to the side, only going as far as comfortable
- Bring the leg back into the starting position, relax
- Repeat 15 times (or as pain allows) every 2 waking hours
3. Strength: aim to do 4 times per day
- Static quads
- Long sit with your back supported and legs out straight
- Place a pillow or folded towel underneath your operative leg knee
- Gently press the knee in towards the bed by tensing your thigh muscles and bringing your toes back towards you
- Hold for up to 5 seconds, relax
- Repeat until your muscles feel tired

- Static glutes
- Long sit with your back supported and legs out straight
- Tense/squeeze your buttock muscles together
- Hold for up to 5 seconds, relax
- Repeat until your muscles feel tired
Phase 1: Week 1-2
Aims:
- To reduce pain and swelling
- To start to regain some range of movement back into the hip
- Begin basic strengthening exercises to activate the muscles surrounding the hip
Criteria to enter phase 1:
- Discussion with your Physiotherapist about progression to phase 1
- Wound healing well with no signs of infection
- Reduction in pain and inflammation
- Beginning to weight-bear more using the assistance of your crutches/walking aid
1. Walking:
- Your Physiotherapist will advise you on the type of walking aid you should be using at this stage.
- Whilst awaiting a hip replacement, individuals will often develop a limp to try and reduce the amount weight being placed through their sore hip. After the operation it is therefore important to begin working towards having a good walking pattern, making sure not to limp
- Always wear good supportive footwear
2. Mobility: continue with the circulation and mobility exercises from the immediate post-op phase:
- Ankle pumps and circles
- Hip flexion- heel slides
- Hip abduction
Add in the following standing exercises as advised by your Physiotherapist. Complete every 2 waking hours, 5 days per week. Keep each exercise within the range that is comfortable for you.
- Hip flexion in standing
- Stand upright with support
- Bring your knee up towards your chest- do not go past 90 degrees/hip height
- Relax your leg back to the starting position
- Repeat 15 times (or as pain allows)
- Hip abduction in standing
- Stand upright with support
- Keeping your leg straight and toes pointing forwards, lift your leg out to the side
- Relax your leg back to the starting position
- Repeat 15 times (or as pain allows)
- Hip extension in standing
- Stand upright with support
- Keeping your leg straight and toes pointing forwards, lift your leg out behind you
- Relax your leg back to the starting position
- Repeat 15 times (or as pain allows)

3. Strength: complete 3-4 times per day, 5 days per week. Perform exercises in long sitting with your back supported and legs out straight.
Continue with the strengthening exercises from the immediate post-op phase:
- Static quads
- Static glutes
Add in the following exercises:
- Inner range quads
- Place a rolled-up towel underneath your operative leg knee
- Tense your thigh muscles to straighten the knee
- Hold for up to 5 seconds, relax
- Repeat until your muscles feel tired
- Static hamstrings
- Bend your operative leg knee and dig your heel in towards the bed tightening the muscles at the back of your thigh- do not flex the hip past 90 degrees/right angles
- Hold for up to 5 seconds, relax
- Repeat until your muscles feel tired

Phase 2: Weeks 3-6
Aims:
- To gradually increase the load placed on the hip joint through progressive strengthening exercises
- Continue to increase the amount of weight placed through your operative leg during walking
Criteria to enter phase 2:
- Discussion with your Physiotherapist about progression to phase 2
- Wound healing well with no signs of infection, stitches/staples removed
- Continued reduction in pain and inflammation
- Mobility has reached goals from phase 1
- Walking: continue to progress as able, working towards having a good walking pattern- make sure not to limp.
- You should continue to use your crutches/walking aid for as long as your Surgeon advises.
2. Cardiovascular work: 3-4 times per week
- Stationary exercise bike: 5-10 minutes
- Keep the resistance LOW
- Ensure the seat is in a high position to avoid hip flexion past 90 degrees
- Be careful when getting on/off the bike to follow your hip precautions
3. Hydrotherapy/pool work: 3-4 times a week (as able).
ONLY if appropriate and ONLY once you have been advised at your review appointment that the wound has healed and that you are allowed to get it wet.
Ensure your Physiotherapist supervises you during the first session and that an aqua belt is worn to support you in the water.
- Aqua walking/jogging: use your arms and legs in the same motion as you would do on land. Aim to do 10 mins in total– increase this by 5 minutes each week.
- Mobility: perform 3 sets of 10 repetitions of the following exercises at the side of the pool (remaining in the water) whilst taking a rest in between sets of aqua walking/jogging.
- Hip flexion– take your knee up towards your chest- do not go past 90 degrees hip flexion/right angles
- Hip extension– take your leg out behind you, keeping the knee straight
- Hip abduction– take your leg out to the side, keeping the knee straight
4. Mobility– continue with the following standing exercises from phase 1.
Aim to complete 15 repetitions (or as pain allows) of each exercise, repeat 2-3 times per day, 5 days per week
- Hip flexion
- Hip abduction
- Hip extension
5. Strength: aim to complete 3-4 times per day, 5 days per week. Perform exercises in long sitting with your back supported and legs out straight
Continue with the following strengthening exercises from phase 1:
- Static glutes
- Static hamstrings
- Inner range quads
Add in the exercises below:
- Straight leg raises
- Keeping your toes pointing to the ceiling, lift your operative leg straight up off the bed
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Straight leg raises with foot pointing outwards
- Keeping your foot pointing outwards (at about 45 degrees), lift your operative leg straight up off the bed
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Hip abduction with resistance- avoid using a resistance band if you have an allergy to latex
- Attach a ½ kg ankle weight around your operative leg or alternatively use a yellow resistance band tied loosely around both ankles (you may need assistance to attach this– do not to bend forward past 90 degrees hip flexion).
- Take your operative leg out to the side as far as comfortable
- Hold for up to 5 seconds then return to starting position
- Repeat until your muscles feel tired

Phase 3: Week 7-12
Aims:
- To continue progressing strengthening exercises adding in resistance if appropriate and advised
- Continue to work on having a good walking pattern
- To begin basic core exercises
Criteria to enter phase 3:
- Discussion with your Physiotherapist about progression to phase 3
- Mobility goals from phase 2 have been reached, with good range into hip abduction being achieved
- Minimal pain during and after physiotherapy exercises and walking
- Walking: gradually increase (as able) the duration and amount of walking you are doing
2. Cardiovascular work: 4-5 times per week.
- Stationary exercise bike: 15-20 minutes
- Keep the resistance LOW and use a high seat position
- Cross trainer: 5-10 minutes
- Begin at 10 weeks +
- Keep the resistance LOW.
3. Hydrotherapy/pool work: continue from phase 2, aim for 3-4 times per week
- Aqua walking/jogging: aim to do 30 minutes in total.
- Mobility: 3 sets of 10 repetitions of each exercise in between sets of aqua walking/jogging:
- Hip flexion
- Hip extension
- Hip abduction
4. Mobility– continue mobility exercises from phase 2
5. Strength: aim to complete 2-3 times per day, 5 days per week. Complete exercises in long sitting with your back supported.
- Discuss with your Physiotherapist before adding in or increasing resistance.
- Make sure to follow your advised hip precautions when attaching the resistance- you may need somebody to assist you with this
- If you have an allergy to latex use ankle weights or latex free resistance bands
- Resistance band colour progression: no band > yellow > red > green > blue > black
- Hip Abduction with resistance– continue from phase 2, increasing the resistance as able.
- Straight leg raises
- Attach ½ kg ankle weights or a yellow resistance band around both ankles
- Keeping your toes pointing to the ceiling, lift your operative leg straight up off the bed
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Straight leg raises with foot pointing outwards
- Attach ½ kg ankle weights or a yellow resistance band around both ankles
- Keeping your foot pointing outwards (at about 45 degrees), lift your operative leg straight up off the bed
- Hold for up to 5 seconds, then relax
- Repeat until your muscles feel tired

- Inner range quads
- Place a rolled-up towel underneath your knees
- Attach ½ kg ankle weights or a yellow resistance band around both ankles
- Tense your thigh muscles to straighten your operative leg knee
- Hold for up to 5 seconds, relax
- Repeat until your muscles feel tired

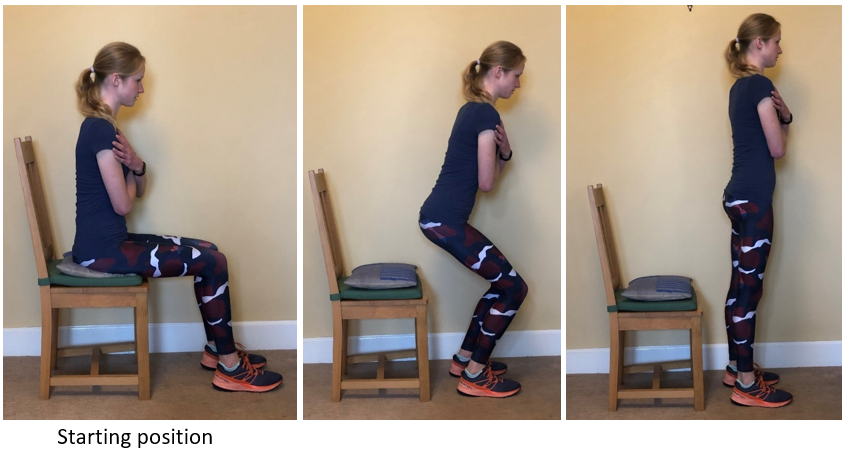
- Sit-to-stand
- Start seated in a chair- make sure the chair is high to avoid your hips being lower than your knees
- With your arms across your body, slowly rise up from the chair
- Once standing, slowly lower yourself back down into the chair without using hands- try to keep the movement controlled
- Repeat until your muscles feel tired
- Double leg heel raises
- Stand upright, feet hip width apart
- Hold onto a stable support in front of you
- Lift both heels off the floor, hold for up to 5 seconds
- Slowly lower to starting position
- Repeat until your muscles feel tired

6. Core exercises: aim to complete 2 times per day, 5 days per week. Work towards holding each exercise for up to 1 minute.
- Double-leg bridge
- Lie on your back with your knees bent
- Flatten the small of your back into the floor and lift your hips up by pushing through your heels
- Concentrate on keeping your hips level and body in a straight alignment
- Plank– begin at 8 weeks post-operation
- Starting on your forearms and knees
- Straighten out your legs to transfer the weight through your forearms and feet
- Concentrate on keeping your back straight by tightening your core muscles
Phase 4: Week 12 onwards
Aims:
- To gradually increase the duration of your walking and cardiovascular exercise
- Continue to progress strengthening exercises by increasing resistance as appropriate
- To begin working towards your functional goals
Criteria to enter phase 4:
- Discussion with your Physiotherapist about progression to phase 4
- Gradual increase in strength with progression onto harder resistance bands or heavier ankle weights
- Good range of motion
- Minimal pain during and after physiotherapy exercises and walking
- Walking: continue to progress as able, gradually increasing your walking endurance
2. Cardiovascular work: continue with cardiovascular work from phase 3, gradually increasing the duration and resistance as advised by your Physiotherapist.
- Stationary exercise bike: use a high seat position
- Cross trainer
3. Continue with hydrotherapy/pool work: aim for 3-4 times per week
- Aqua walking/jogging: 30-minute session
- Mobility: continue with 3 sets of 10 repetitions of the mobility exercises from phase 2 in between sets of aqua walking/jogging.
4. Mobility: continue with your mobility exercises from phase 2
5. Strength: continue with the following resistance exercises from phase 3. Progressively increase the resistance (as able) ensuring that the exercises remain pain free.
Repeat each exercise until your muscles feel tired, 2-3 times per day, 5 days per week
- Straight leg raises
- Straight leg raises with foot pointing outwards
- Hip abduction with resistance
- Sit-to-stand
- Double-leg heel raises: once you can comfortably complete the double-leg heel raises from phase 3 progress to single-leg heel raises.

- Wall slides
- Start with your feet hip width apart, step approx. 1 step away from the wall. Lean your back flat against the wall
- With arms by side, slowly slide down the wall to around 60-80 degrees of hip flexion before sliding back up to the starting position
- Do not perform a deep squat
- Repeat until your muscles feel tired

6. Core exercises: aim to complete each exercise 2 times per day, 5 days per week. Make sure you can hold each exercise from phase 3 comfortably for more than 1 minute before progressing.
- Bridge
- Plank

- Once you can comfortably complete the above core exercises, further progressions and exercises can be found on Frank Gilroy’s Core strengthening programme by clicking here
Return to activity
- Returning to activity after a total hip replacement is different for every individual so it is important to discuss your goals with your Surgeon or Physiotherapist.
- Remaining active by doing low impact activities (as able) is very important as it improves your general health, strength and cardiovascular fitness.
Low impact activities that are advised include:
- Walking
- Golf
- Swimming (avoid breaststroke instead using freestyle/flutter kick)
- Stationary bike
- Cross trainer
- Particular types of dancing (e.g ballroom)
- Bowling
- Increased or prolonged impact, overuse and falls associated with sporting activities can lead to poor long-term outcomes for hip replacements. It is therefore advisable to participate in low or moderate impact activities rather than high impact sports.
- One of the most common questions asked by younger or more athletic individuals is about what sports they are allowed to do following a hip replacement. More information on return to sport can be found here (table on p173). However, it is always best to ask your Physiotherapist directly if there is a particular sport you wish to participate in.
When can I return to work?
Occupational duties and individual factors largely determine the timescale for returning to work after a hip replacement. Jobs that require limited lifting and bending could see patients returning around 3-4 months post-operation but this is a decision that needs to be discussed with your Physiotherapist.
You must consult a chartered Physiotherapist or your specialist before embarking on this programme. If you do experience pain or discomfort as a result of any of the exercises, stop immediately and speak to a health professional.
{kind=link}
{kind=link}
{kind=link}