A patient guide to physiotherapy for shoulder pain and/or stiffness

Frank Gilroy- Consultant Physiotherapist
Megan Thea Ross Browne- Student Physiotherapist
Contents
- Anatomy of the shoulder
- What might cause shoulder pain and stiffness?
- What is a frozen shoulder?
- Symptoms of a frozen shoulder
- Why does a frozen shoulder develop?
- Diagnosis
- Recovery
- Phases of a frozen shoulder
- Rehabilitation:
- Painful/early phase- preventing stiffness
- Middle/freezing phase- maintaining movement
- Thawing/late phase- regaining movement
- Surgery
- References
Remember this programme is only a guideline. You may progress more rapidly or slowly through the programme as guided by your Physiotherapist. You should always check with them before progressing onto the next rehabilitation stage.
Anatomy of the shoulder
The shoulder is a ball-and-socket joint formed between the head of the humerus (upper arm) and the shoulder blade. It is considered to be one of the most complex joints in the human body.
With a wide and varied range of movement the shoulder is a very mobile joint. This allows you to complete essential tasks within day-to-day life such as getting dressed or washing your hair.
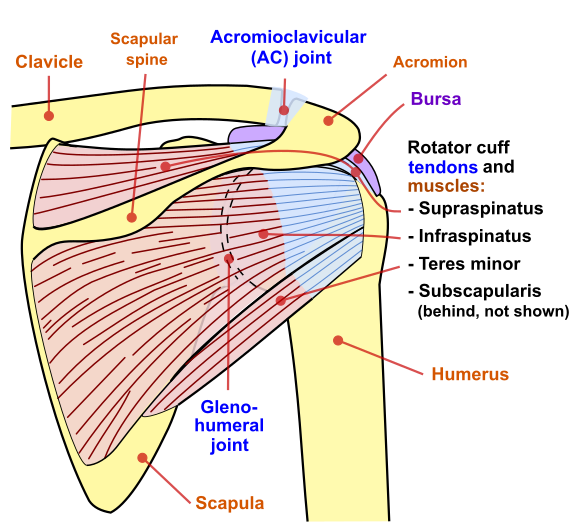
Anatomy of the Shoulder
The shoulder is one of the 4 separate joints that make up the shoulder complex/pectoral girdle. The function of the shoulder complex is to attach the upper limb to the trunk of the body and it consists of the following 4 joints:
- Glenohumeral (shoulder) joint
- Acromioclavicular (AC) joint- formed between the lateral (outer) end of the clavicle and the acromion of the scapula (shoulder blade)
- Sternoclavicular joint- formed between the medial (inside) end of the clavicle and the sternum
- Scapulothoracic joint- where the scapula meets with the ribs on the back of the chest
There are 4 short muscles called the rotator cuff that insert into the shoulder joint. These muscles play an important role in stabilising the shoulder when the arm is moving. The shoulder joint itself is surrounded by a loose fibrous capsule with which the ligaments of the shoulder blend, strengthening it. This capsule is filled with a lubricant called synovial fluid which helps the joint to move smoothly. It is changes to both the joint capsule and synovial lining that can lead to the development of conditions such as a frozen shoulder.
What might cause shoulder pain and stiffness?
Shoulder pain and stiffness is a very common joint complaint that can develop for a number of different reasons. However, the 4 main causes of a painful shoulder are:
Trauma/injury– this could be either acute trauma (for example, injuring your shoulder in a car accident) or trauma from a previous accident/injury
Overuse- related to either a sudden increase or change in activity. Common overuse conditions include shoulder impingement, bursitis and tendonitis.
Degenerative changes- conditions commonly associated with increased age for example, osteoarthritis or rotator cuff disease
Post-operative: pain and stiffness that can persist after shoulder surgery

What is a frozen shoulder?
Frozen shoulder (also called adhesive capsulitis) is a common shoulder disorder that is characterised by pain, stiffness and the progressive loss of shoulder movement. It can occur at any age but is more common in those over the age of 40 and affects women more than men. Individuals with medical conditions such as diabetes can also be at increased risk of developing a frozen shoulder.
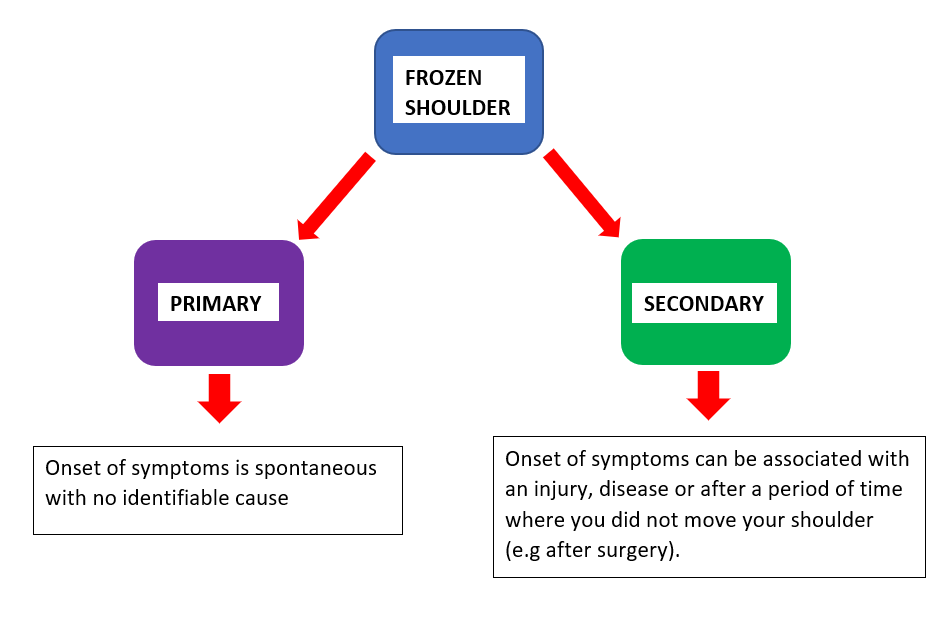
A frozen shoulder can be classified as being of either primary (idiopathic) or secondary onset:
Symptoms of a frozen shoulder
The main symptoms are:
- Pain on the outside of the upper arm- this can spread from the neck area down into your arm depending on the severity of the inflammation.
- Pain on movement
- Stiffness and loss of movement– certain movements become difficult initially, such as putting on a bra or washing your hair
- Night pain and sleep disturbance– due to difficulty lying on the affected shoulder
Why does a frozen shoulder develop?
Frozen shoulder develops when the tissue that surrounds the shoulder joint becomes inflamed and painful. The inflammation can cause the tissue (in particular the joint capsule) to become tighter and shrink, making it harder to move your arm.
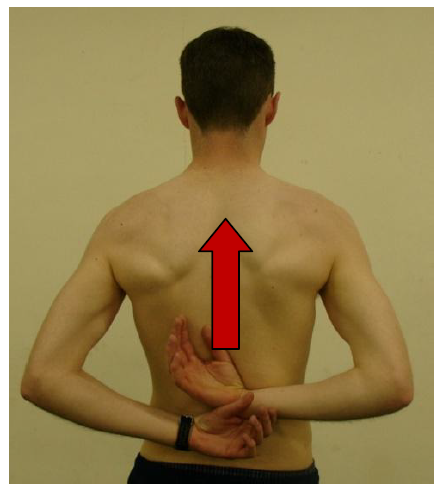
The natural response to the pain is to stop moving the shoulder normally as movement will typically cause more discomfort. Often people will start holding the affected arm in a protective position as shown in the image below.

When the structural changes occurring within the joint are combined with the lack of movement, the shoulder gradually becomes increasingly stiff and sore.
Diagnosis
A clinical assessment will be made by your Doctor or Physiotherapist who will look out for the main signs of the condition. Symptoms often develop gradually, but an early diagnosis can enable you to start exercises that will help to keep your shoulder moving and reduce pain.
Recovery
The natural timescale for recovery can vary for each individual from between 6 months- 2 ½ years. However, almost all frozen shoulders will resolve over time with nature and through following an exercise regime.
Phases of a frozen shoulder
The natural progression of frozen shoulder has 3 main phases as shown in the graph below. Generally- as pain increases, movement decreases then as movement increases, pain decreases.
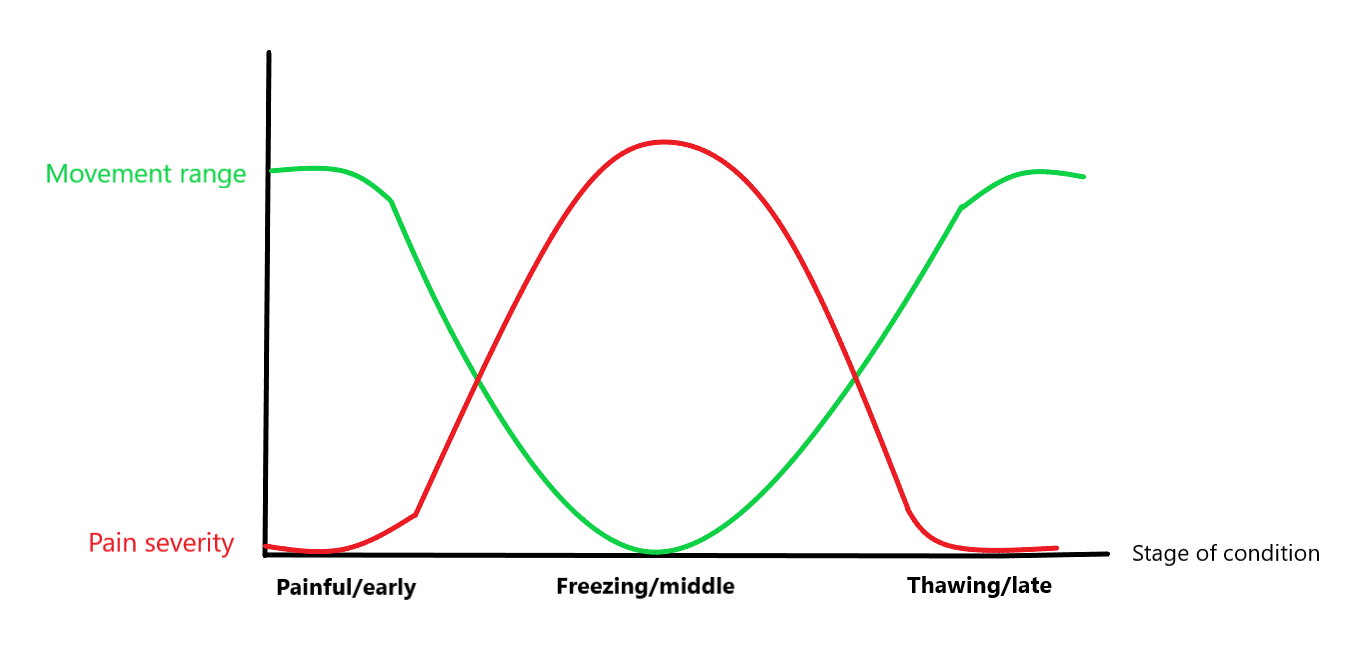
- Painful/early phase
- Gradual onset of pain (dull aching at rest)
- Initially, any loss of movement often goes unnoticed until everyday activities (e.g reaching up into cupboards) become increasingly difficult.
- Pain at night and sleep disturbance
- Freezing/middle phase
- Shoulder becomes increasingly stiff in all directions of movement
- Pain may gradually begin to reduce
- Thawing/late phase
- Movement of the shoulder slowly improves and there is a continued reduction in pain
Normally, people will regain movement in their shoulder but this can take a considerable amount of time.
Rehabilitation
Rehabilitation for frozen shoulder corresponds with the 3 phases of the condition described above:

There is not considered to be one optimum treatment pathway for frozen shoulder therefore, it is important to discuss all treatment options with your Doctor or Physiotherapist and follow their advice.
Set timescales for each rehabilitation stage have not been provided within this guide as the progression of the condition can differ between individuals. Doing your physiotherapy exercises will help you to move through the phases.
IMPORTANT: before starting this programme, please note that:
- Progressions throughout the programme, between and within phases, should be made only when advised by your Physiotherapist
- If at any point during your programme you begin to experience worsening pain, stop the exercise and consult your Doctor or Physiotherapist
Painful/early phase- preventing stiffness
Aim: to use physiotherapy exercises to reduce pain and prevent restriction of shoulder movement
Goals:
- To try and prevent shoulder stiffness from increasing by doing your exercises regularly
- To avoid irritating the joint by keeping shoulder movements within your pain-free range
- To discuss pain-relief options with your Doctor to help manage your symptoms
Pain management:
- Pain-relief medication and/or anti-inflammatory tablets might be recommended by your Doctor
- Steroid injection– might be advised if the pain continues, however injections are not suitable for everyone and cannot be given to those with certain medical conditions.
- Activity modification– try to modify or avoid movements that cause you pain however, it is important to keep using and moving your shoulder as able.
Exercises
Pendular exercises: mobility exercises to keep your shoulder moving
- Perform each of the following exercises within the limits of your pain
- Repeat each exercise 20 times. Aim to do them 4 times per day, 5 days per week
1. Lean over a stable table, supporting yourself with your unaffected arm
Let your affected arm hang down
Swing the arm forwards and back

2. Lean over a stable table, supporting yourself with your unaffected arm
Let your affected arm hang down.
Swing the arm side to side

3. Lean over a stable table, supporting yourself with your unaffected arm
Let your affected arm hang down.
Swing the arm in circular motions clockwise and then anti-clockwise

Active assisted exercises: to maintain shoulder range of movement
- Only go as far as is comfortable- don’t force your shoulder
- Repeat each exercise 10 times. Aim to do them 3 times per day, 5 days per week
- Try to hold the end position of each exercise for up to 5 seconds
- Lying flat. Keep your elbows into the side at 90 degrees and use a stick to gently stretch the arm, rotating outwards.

2. Lying flat, use your unaffected arm or a stick to gently stretch the arm above the head.

3. Using the stick lift both arms away from the body behind your back.

4. Stand facing a wall. Try to walk your fingers up the wall as far as possible and then walk your fingers back down the same way.
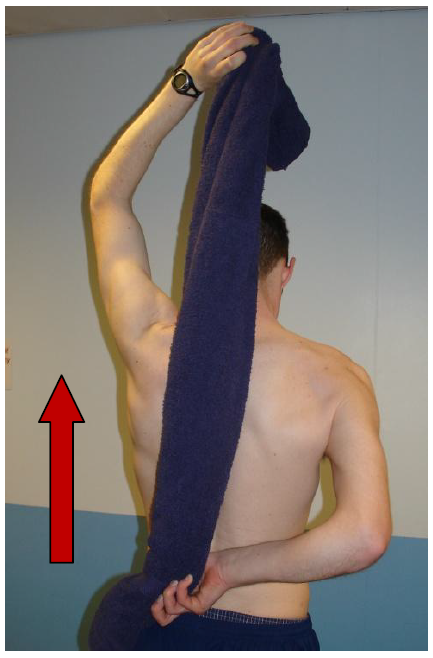
5. Using the unaffected arm or a towel, assist your affected arm as far up your back as able
Freezing/middle phase: maintaining movement
Aim: to maintain the shoulder movement you currently have until your pain begins to reduce.
Goals:
- To keep exercises within your pain free range to prevent further irritation of the shoulder
- To minimise any further loss of movement
Pain management:
- Stronger pain and swelling relief may be prescribed (if appropriate) by your Doctor for a short period of time to help manage your symptoms.
- Heat: apply a heat pack (e.g a hot water bottle) over the painful area for 15-20 minutes before doing your exercises. This can help to ease stiffness.
- Do not apply the heat directly to the skin (wrap in a towel) to prevent burning the area
Exercises:
Too much physiotherapy can irritate your shoulder during the middle phase therefore, it is important not to force exercises beyond your pain-free range as this can cause shoulder stiffness to increase.
Pendular Exercises: continue with the following pendular exercises from the early phase:
Repeat each exercise 20 times. Aim to do them 4 times per day, 5 days per week.
- Backwards and forwards
- Side-to-side
- Circular
Active assisted stick exercises: continue with the following exercises from the early phase:
- Only go as far as is comfortable- don’t force your shoulder
- Repeat each exercise 10 times. Aim to do 3 times per day, 5 days per week
- Try to hold the end position of each exercise for up to 5 seconds
- Lying flat. Keep your elbows into the side at 90 degrees and use a stick to gently stretch the arm, rotating outwards.
2. Lying flat, use your unaffected arm or a stick to gently stretch the arm above the head.
Add in the following exercise:
3. Table flexion slides
- Sit at a table with a folded towel or dishcloth in front of you
- Place both hands on the towel and slowly slide it away from you
- Once you have gone as far as is comfortable, keep your hands in contact with the towel and slide it back towards you
- Repeat 10 times, 3 times per day, 5 days per week

Thawing/Late phase: regaining movement
Aim: to use physiotherapy exercises to regain shoulder movement once your pain has reduced
Goals:
- To regain shoulder movement
- To begin using and strengthening the muscles around your shoulder
Pain management:
- You can continue to use heat for pain relief if helpful (see middle phase)
Exercises
Active-assisted exercises
- Only go as far as is comfortable- don’t force your shoulder
- Repeat each exercise 10 times. Aim to do 3 times per day, 5 days per week
Continue with the following exercise from the middle phase:
- Lying flat. Keep your elbows into the side at 90 degrees and use a stick to gently stretch the arm, rotating outwards.
Add in the following exercises:
2. Using the stick lift both arms away from the body
3. Using the unaffected arm or a towel, assist your affected arm as far up your back as able. Only go as far as comfortable. Try to hold the end position for up to 5 seconds. Repeat 10 times.
4. Stand facing a wall
- Slide your hands up the wall, slide them out to the side, then down (in a circular movement)
- Each time try to make the circle slightly bigger
- You can reverse the direction half way through
- Repeat 10 times

Strengthening
It is important to strengthen your shoulder over the longer term. You will begin to regain strength just from using your shoulder for daily activities and tasks again.
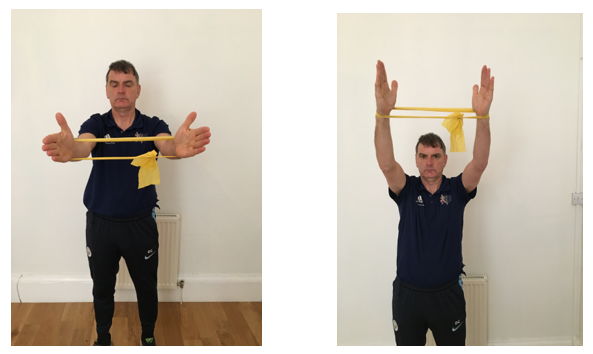
- Shoulder elevations
- Start by using a yellow theraband.
- Tie it in a loop so that you can place it around both of your forearms
- Straighten out your elbows and pull your arms outwards until you feel the resistance of the band
- Lift both arms up in front of you, going as far as you can.
- Make sure you keep the resistance on throughout the movement
- Repeat 5-10 times, 2 times per day
- If you have an allergy to latex make sure you use latex-free resistance bands
- Resistance band colour progression: yellow > red > green > blue > black
Stretching
Aim to do the following exercises 3 times per day, 5 days per week
- Place both hands on a stable table
- Walk your feet backwards, bending at the waist to stretch out your shoulders
- Hold this position for up to 5 seconds
- Repeat 10 times
- Try to bend a little further at your waist each time to increase the stretch

2. Stand facing a door frame
- Bend the elbow of your affected arm to 90 degrees/right angles and keep it by your side throughout the exercise
- Place the palm of your affected arm against the door frame so that it cannot move during the exercise
- Turn sideways away from the door, rotating your body away from the frame
- You should feel a stretch on the inside of your shoulder
- Hold for up to 30 seconds
- Repeat 3 times
Click here to view a video of specific exercises within this guide
Surgery
Surgical treatment of frozen shoulder is uncommon with the timing of intervention controversial. Non-operative treatment will be tried before surgery is considered. However, if symptoms show no sign of improvement after 9-12 months and the shoulder remains stiff and painful, your GP/Doctor may discuss surgery with you.
Early surgical intervention can occasionally be considered for individuals with:
- High risk factors, for example diabetes
- Chronic unresolving symptoms
- Bilateral symptoms (both shoulders)
The aim of surgery is to release the contracted joint capsule to allow better movement.
Two of the main surgical techniques used for frozen shoulder are:
- Hydrodilatation
- Capsular release
Hydrodilatation is performed by a Radiologist under a local anaesthetic (where you remain awake). The Radiologist uses x-ray guidance to inject a mixture of sterile saline, local anaesthetic and steroid into the shoulder joint. The injection aims to stretch out the adhesions within the joint capsule, reducing inflammation and improving range of movement.
For exercises that are to be started 2 days after your hydrodilatation procedure click here
Shoulder capsular release involves a surgeon using arthroscopic techniques (keyhole surgery) to release the tight capsule that develops with a frozen shoulder. Performed under a general anaesthetic (where you are asleep), the surgeon will inspect the shoulder joint for typical features of the condition. Different portions of the contracted capsule will then be cut to increase volume and improve movement. Additionally, a gentle manipulation is performed to complete the release. Usually, this procedure will give an immediate return to normal range of movement.
After either procedure, intensive physiotherapy is required to maintain the increased movement that is gained through surgery.
References:
BROOKSBANK, A., 2012. Shoulder anatomy: resources [online]. Painfulshoulder. [viewed 16 August 2020]. Available from: https://painfulshoulder.co.uk/resources/shoulder-anatomy/
CHAN, H.B.Y., PUA, P.Y. & HOW, C.H., 2017. Physical therapy in the management of frozen shoulder. Singapore Medical Journal [online]. 58(12), pp.685-689. [viewed 8 October 2020]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5917053/
CLINICAL EDGE, 2020. Stiff shoulder- Risks & culprits, Stuck on the Stiff Shoulder? Freeing up your assessment & treatment. [viewed 28/08/2020]. Available from: https://www.clinicaledge.co/stiffshoulder1?utm_source=ActiveCampaign&utm_medium=email&utm_campaign=ACSSSPLC3&utm_term=frozenshoulder&vgo_ee=0Br5wHO7Vf%2FhDHmBbofUOr35hO7C%2FF3J%2FgQB9Uu3XAY%3D
DENNIS, L., BREALEY, S. & RANGAN, A., 2017. Managing Idiopathic Frozen Shoulder: A survey of Health Professionals Current Practice and Research Priorities. Shoulder and Elbow [online]. 2(4), pp.294-300. [viewed 19 August 2020]. Available from: https://doi-org.gcu.idm.oclc.org/10.1111%2Fj.1758-5740.2010.00073.x
ELJABU, W., KLINGERM H.M. & KNOCH, M.V., 2016. Prognostic factors and therapeutic options for treatment of frozen shoulder: a systematic review. Orthopaedic Surgery [online]. 136(1), pp. 1-7. [viewed 26 August 2020]. Available from: http://dx.doi.org.gcu.idm.oclc.org/10.1007/s00402-015-2341-4
JMARCHN., 2018. Shoulder joint back-en.svg [online image]. [viewed 21 February 2021]. Available from: http://commons.wikimedia.org/w/index.php?curid=67117834
NATIONAL HEALTH SERVICE, 2018. Frozen shoulder [online]. National Health Service. [viewed 18 August 2020]. Available from: https://www.nhs.uk/conditions/Frozen-shoulder/
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE., 2017. Scenario: Frozen Shoulder [online]. National Institute for Health and Care Excellence. [viewed 11 October 2020]. Available from: https://cks.nice.org.uk/topics/shoulder-pain/management/frozen-shoulder/
NORRIS, C.M., 2018. Sports and Soft Tissue Injuries: A Guide for Students and Therapists. 5th ed. Taylor & Francis Group.
PALASTANGA, N., SOAMES, R. & PALASTANGA, D., 2008. Anatomy and human movement pocketbook. Churchill Livingstone Elsevier.
RYAN, V., BROWN, H., LOWE, C.J.M. & LEWIS, J.S., 2016. The pathophysiology associated with primary (idiopathic) frozen shoulder: A systematic review. BMC Musculoskeletal Disorders [online]. 17(1), p.340. [viewed 18 August 2020]. Available from: https://doi.org/10.1186/s12891-016-1190-9
SHAYNE_ch13., 2016. Shoulder pain [online image]. [viewed 09 October 2020]. Available from: https://www.freepik.com/free-photo/shoulder-pain_905860.htm#page=1&query=shoulder&position=10
STANDRING, S., 2008., GRAY’S Anatomy: The Anatomical Basis of Clinical Practice. 40th ed. Churchill Livingstone Elsevier.